

Finland Published the Data (Part I): What the Study Found
A national registry spanning more than two decades. Every patient tracked. No one forgotten about.

The numbers
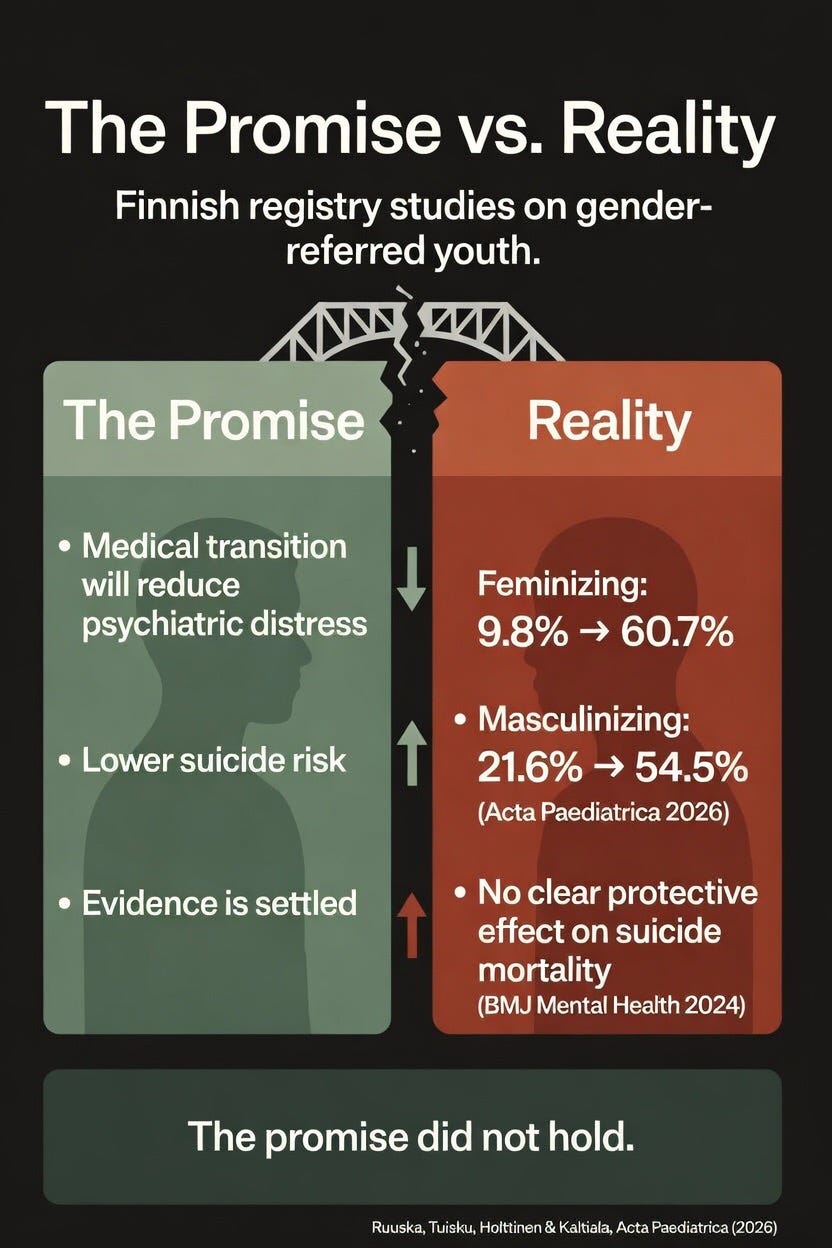
Start with the number about medicalization, the one that ends the argument: among the boys who underwent feminizing gender reassignment, the rate of serious psychiatric illness rose from 9.8% before referral to 60.7% afterward, a more than sixfold increase. For girls who underwent masculinizing gender reassignment, it rose from 21.6% to 54.5%.
These are the children who, by clinical standards, looked like good candidates for medical intervention. They were selected for treatment because their psychiatric needs were far lower at intake than gender-dysphoric youth who were not selected. Yet after treatment, more than half of the medicalized patients required specialist-level psychiatric care. Their rates of psychiatric morbidity had approached those of their gender-dysphoric cohorts who had been judged not mentally well enough to be medicalized. And it was not just the medicalized patients. The pattern ran deeper than that.
The overall picture
Gender-referred adolescents were roughly three times as likely as their matched peers to have serious psychiatric illness before they ever walked into a gender clinic (45.7% versus 15.0%), and more than four times as likely two or more years afterward (61.7% versus 14.6%). The control population held flat across the same period. That stability matters: if the rising psychiatric numbers among gender-referred adolescents reflected only improved screening or expanded access to care, a comparable increase would be expected in the matched controls. None appeared.
What the study measured and why it matters
The study was published in the peer-reviewed Nordic pediatric journal Acta Paediatrica, and led by Finnish researcher Sami-Matti Ruuska and senior author Riittakerttu Kaltiala. It drew from Finland’s national health registries to follow every individual under 23 referred to the country’s two centralized gender identity clinics between 1996 and 2019: 2,083 gender-referred individuals matched against 16,643 peers from the general population. Each case was matched to four male and four female controls by birth year and municipality, so that every gender-referred individual could be compared against peers of the same age from the same area who had not been referred.
Dr. Julia Mason, a board-certified pediatrician and founding board member of the Society for Evidence-Based Gender Medicine, put it concisely: “The Finns went into providing GAC to minors with an open mind, but unlike some clinics, they paid attention to how things were going.” Kaltiala has said, as she has recounted in interviews, that when her superiors told her to open a pediatric gender clinic in 2011, she reviewed the literature and was not particularly impressed. But Finland is a small country, she noted, and everyone else seemed so confident. So she followed the Dutch protocol, quickly observed that the patients arriving at her clinic did not match the profile described in the Dutch research, and began publishing what she found.
Dr. Yuan (Ray) Zhang, a health research methodologist at McMaster University and co-author of the HHS evidence review on pediatric gender dysphoria, assessed the study’s design: “It is a national registry so it is not selective in recruiting study participants. It compares treated with untreated youth with gender dysphoria. It has long-term follow-up. Due to these features, it has arguably better study design than other studies in this field.” Zhang also flagged a genuine limitation: the study’s starting point for measurement (its ‘index date’) is the first clinic appointment, not the start of treatment, meaning the two-year waiting period before the researchers began counting outcomes may capture different amounts of post-treatment time for different patients. In some cases, treatment may not yet have begun within that window, meaning the ‘after’ measurement could predate the intervention it is meant to follow.
Because Finland’s health registers are mandatory and patients cannot opt out, the dataset captured the complete trajectory of every gender-referred adolescent in the country over that period. The median follow-up (the length of time each patient was tracked) was just under five years, with a maximum of twenty-five.
What the study tracked was contact with specialist-level psychiatric services. In Finland’s two-tiered mental health system, primary care handles routine psychiatric conditions, including prescribing antidepressants and managing common diagnoses like ADHD. Patients are referred to specialist-level services only when their condition is severe enough, or deteriorating enough, that primary care cannot manage it. Once stabilized, they return to primary care. The study tracks only this upper tier. As Mason explained: “Routine primary care psychiatry, such as managing ADHD or simple depression with an SSRI, is not handled by ‘specialist-level psychiatric’ services in Finland.” What the study captures is not routine mental health contact but a threshold of severity that required referral.
Medical gender reassignment was defined as masculinizing or feminizing hormone treatment lasting at least a year, chest masculinization surgery, and/or genital surgery. Of the 2,083 gender-referred individuals, 38.2% (796) proceeded to medical gender reassignment.
The researchers compared rates of specialist-level psychiatric treatment at two time points: before the first appointment at the gender identity clinic, and from two years after that appointment onward.
The two-year gap allowed for the assessment process and for any subsequent medical intervention to get underway before measuring outcomes. The “after” window ran from that two-year mark through to the end of observation (death or June 2022), meaning the follow-up period varied by individual.
Upending the minority stress model
The prevailing model in gender-affirming care holds that psychiatric distress in gender-dysphoric youth is secondary to the gender dysphoria itself, driven largely by social stigma and prejudice. Under this model, treating the dysphoria through medical transition should alleviate the psychiatric problems. The Finnish data shows the opposite.
The proportion of gender-referred adolescents who had already required specialist-level psychiatric treatment before their first contact with gender identity services doubled from the earlier cohort to the later one: 23.7% in 1996 to 2010 versus 47.9% in 2011 to 2019. The general adolescent population showed no comparable rise. “Minority stress theory posits that mental disorders in transgender identifying people largely arise from actual and internalised prejudice. With the opening up of society with regard to sexual and gender minorities, a decrease in psychiatric morbidity might have been expected in the later GD cohorts,” the authors write. They acknowledge that reduced stigma may increase treatment-seeking, but if that were the full explanation, the newer cohorts would look broadly similar to the earlier ones, just larger. Instead, the psychiatric profile of the population contacting gender services became dramatically heavier over time.
The authors’ conclusion inverts the prevailing model: “The considerable severe psychiatric morbidity prior to contacting the GIS, and its increase over time, suggest that for some of these adolescents, GD may be secondary to other mental health challenges.” Causality, they suggest, may run the other way, with psychiatric difficulties giving rise to gender-related distress rather than vice versa.
How the treatment comparison worked
The study divided the gender-referred adolescents into two groups: those who went on to receive medical gender reassignment, and those who did not. Among those who did not medicalize, psychiatric illness rates before referral were high: 53.1% among males and 65.0% among females. In Finland, patients with the most severe psychiatric conditions are not approved for medical gender reassignment. The sickest patients were, by design, kept out of the treatment group. Among those who did medicalize, initial rates were much lower: 9.8% for males and 21.6% for females. The authors note that the pre-referral psychiatric treatment rate for the males who later underwent feminizing treatment was not significantly different from the control males. These boys entered the system looking psychiatrically ordinary. More than 60% of them did not stay that way.
The study’s authors observe that estrogen has been found to potentially cause depressive symptoms, and that while masculinizing hormones may temporarily improve mood, psychiatric treatment needs were also markedly increased among those who received them. Dr. Roy Eappen, a Montreal endocrinologist and assistant professor of medicine at McGill University, confirmed that this pattern is consistent with established endocrine knowledge: “Estrogen in men is usually a cause of fatigue, low energy, gynecomastia [breast tissue development] and sexual dysfunction.” He noted that testosterone may improve mood in women but is “certainly not a treatment for depression.” Eappen also pointed to a grim historical parallel: “We would note that estrogen has been used as a punishment for gay men in the past. Alan Turing, a hero of World War II and a gay man, was given estrogen, and that likely contributed to his untimely end.” The precise cause of Turing’s death remains debated among historians, but the psychiatric effects of the estrogen treatment he was subjected to are not.
When the authors adjusted their analysis to account for prior psychiatric treatment, birth year, and year of referral, the apparent differences between medicalized and non-medicalized groups vanished. All gender-referred groups showed similarly elevated risk of subsequent psychiatric treatment compared to the general population: roughly five to six times higher than male controls and three to four times higher than female controls, regardless of whether they had medicalized. In other words, once the researchers accounted for the fact that the untreated group started out sicker, treatment status made no difference to the outcome.
Zhang assessed the convergence finding with characteristic methodological care: “It does raise the question that if the medical reassignment is effective in improving mental health, why this is not seen in a large national registry.” And among some individuals who received it, the authors conclude, it appears linked to deterioration in mental health.
In Part II: the campaign to discredit the study, the media outlets that said nothing, and what both sides keep getting wrong.